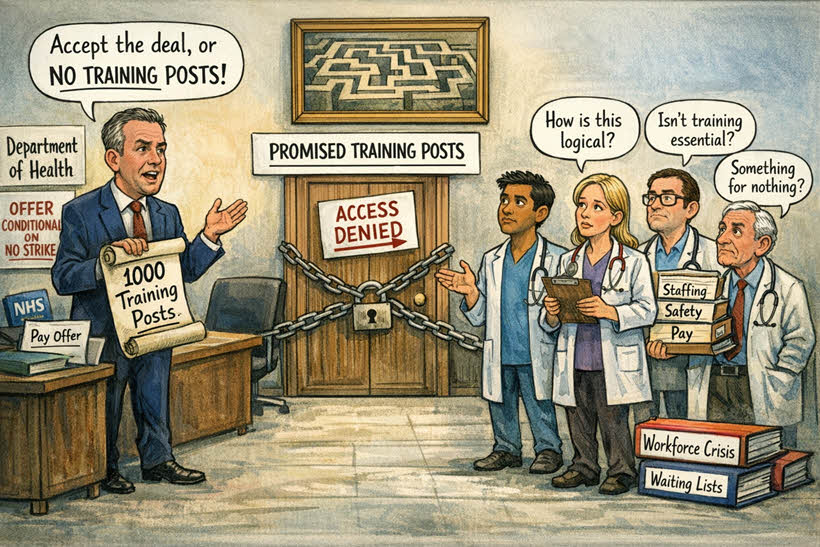
In the continuing chronicle of Britain’s health‑service governance, the latest development arrives with all the subtlety of a departmental memo announcing that oxygen will henceforth be rationed. The Health Secretary, Wes Streeting, has declared that the thousand additional specialty training posts—previously heralded as a strategic investment in the future workforce—will now be contingent upon resident doctors refraining from industrial action (in BMJ). This conditionality is presented not as coercion but as a sophisticated mechanism of partnership, a term which here appears to mean that one party dictates terms while the other is invited to be grateful.
But the logic – if you can call it that – bears an uncanny resemblance to the Trumpian doctrine of conditional generosity, most vividly displayed in the administration’s dealings with Iran. There, too, the offer of reconciliation was framed as a benevolent gesture contingent upon submission: accept the deal or face obliteration. Streeting’s domestic variant replaces missiles with training posts, but the rhetorical architecture is identical—an ultimatum dressed as magnanimity, a partnership defined by asymmetry. In both cases, the power to grant what should be ordinary—security for a nation, stability for a workforce—is transformed into a theatrical instrument of control.
Streeting explains to Parliament that NHS trusts required “arm twisting” to accept the very training posts the government had already promised, a revelation that raises the intriguing possibility that the nation’s hospitals are unconvinced of the utility of having more doctors. He further notes that trust leaders harbour reservations about the “conduct” of resident doctors, though the precise nature of this conduct remains undefined. One might infer that raising concerns about patient safety, staffing shortages, and pay erosion constitutes behaviour unbecoming of medical professionals.
The doctors, for their part, respond with the predictable lack of enthusiasm. They appear perplexed that the provision of adequate training capacity is being treated as a discretionary reward rather than a structural necessity. Several point out that in a health system serving an ageing and increasingly unwell population, the idea that additional training posts require justification is a conceptual innovation of considerable boldness. Others question how the Secretary’s invocation of “something for nothing” aligns with the reality of doctors working nights, weekends, and holidays while waiting lists exceed seven million.
The Department of Health contributes its own clarifying statement, explaining that creating a thousand posts “in a week” is logistically impossible during strike action. This is a compelling argument, though it does not entirely address why the posts—promised months earlier—must be conjured within this particular seven‑day window, nor why their existence depends on the absence of industrial action rather than on workforce need.
Thus the situation resolves into a familiar tableau: a government insisting that its conditional offer is an act of generosity, a medical workforce observing that the conditions themselves undermine the purpose of the offer, and a health system caught between the two, waiting patiently for someone to remember that patients exist.